Neural Circuit Integration
A Neuroscience-Informed Framework to Refine, Extend & Unify Effective Trauma Therapies
The New Neuroscience
Government programs in connecting electronics and photonics directly to human brains have led to a renaissance in understanding how information is stored and processed in the human cortex and surrounding cognitive machinery. Neuroscience is undergoing a fundamental transformation, growing from experimental science into an engineering discipline with large scale machinery interfaced directly to the human Cortex for the first time. Millions of neurons are now routinely observed “thinking” in real-time offering a renaissance in understanding exactly how information is represented and processed in the brain. In order to create interfaces that passed information into and out of the human cortex, it was necessary to develop a deeper understanding of the fundamental physics and algorithms of data encoding in how, exactly, information is represented in, and transported across, the brain –- and not just in terms of general operating principles and large-scale connections which have been the subject of the last few decades of neuroscience research, but with specific transcoding algorithms allowing us to translate directly between patterns of neural firings in the auditory cortex, and music and speech recordings in an MPEG digital format, or between neural patterns in the visual cortex, and digital video files of those images sensed and imagined in the brain. “What I cannot create, I do not understand.” ~ Richard Feynman
With such fantastic new tools, came revolutionary new discoveries in how, not just sensory information, but even abstract ideas and concepts such as benefit, harm, love and hate, and all the myriad ideas represented in our languages, are represented in the brain. These discoveries are now driving a whole new industry in connecting electronics and optics directly to the brain and peripheral nervous system, and also, it turns out, led directly to the new renaissance in AI capabilities where the newly discovered information architecture of the human brain informed a revolution in the new Generative AI models that rely on digital simulations of that same data representation. In this document we review and apply, these new discoveries to better understand the practice, and unusual efficacy of traditional EMDR and other trauma informed therapy modalities, and to design important refinements and extensions of traditional practices to create a new Neural Circuit Integration Therapy model that unifies them all in a cohesive and logically consistent framework.
1.1Cortical Information Storage
The most important new discovery revealed by the latest whole-brain imaging experiments is that the whole brain is involved, and participates in, the representation and processing of every individual concept and abstraction. The traditional ideas of left vs. right brain, and/or localized memories have been definitively disproven. 65,93,94,137 We now have live scanned evidence of exactly how the brain represents information and can directly image what someone is preparing to say or has just heard, or even what they are visualizing from memory. The actual structure of information storage is almost the exact opposite of what the old left-versus right brain simplified analogy of the last century might suggest. The old model postulated that each concept was represented by a specific location in the brain, and that some more creative concepts and cognitive habits resided largely on one side or the other –- for example: left-side = logical/deterministic, right side = emotional/creative. On the contrary, it turns out that our new mass-action measurement tools were finally able to discern the large-scale activity
of the brain in aggregate, and for the first time, definitively show that any single concept is actually represented by the distributed mass action of the entire cortex.
1.2Representation of Information in the Cortex
As described brilliantly by the groundbreaking work of UC Berkeley’s Jack Gallant and Carnegie Mellon’s Marcel Just (both recipients of DARPA | Biological Technologies Office funding), any thought or concept is represented in the brain by the collective action of the
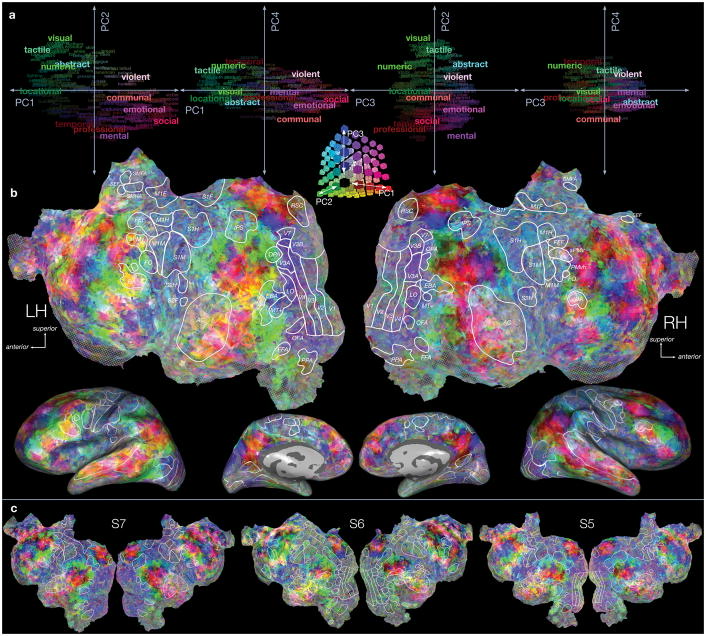
entirety of the cortex, with the relative excitation of each individual area with respect to the other cortical areas, all collectively defining the concept in concert. 93,94 It turns out that each of the different regions of the brain represent a huge range of individual, complex multi-sensory and cognitive information aspects of the experience. Some brain regions are related to sensory experience (sight, sound, smell, taste, touch, proprioception–-the state and positioning of the body–-anything related to that thought, social aspects, location, timing, whether you were hot or cold, or wet, how you felt and your emotional state.) The entirety of your neocortex is involved in representing every individual thought.
For example, when you think of “A dog” you also have related to that concept, the parts of your brain that represent how that dog looks, smells, the feel of its fur or cold nose or teeth, how it moves, the sound of its bark and motion, whether you like or fear that particular dog or dogs in general, links to prior memories and experiences with dogs, dogs from your past life. The very idea of “Dog” is represented in your brain by the relative collective action of all the different areas of your brain that each represent a unique aspect. Your Hippocampus has created a neuron or neurons which link all the different areas of your brain, with the precise connection strengths to each area so that that collective activity across all of those areas in just the right proportions represents “Dog.” 61,198,199 So it turns out that any concept, a rose, or dog, or car, and even abstract ones like harm or benefit, or friend or enemy, truth, or justice–-can be represented by the relative activation of the different areas of the cortex. In a series of brilliant experiments, Just and Gallant determined that over 10,000 different concepts can be uniquely disambiguated by measuring the relative activation of only 70 different, roughly cubic centimeter areas that collectively encompass the entire volume of the cortex.
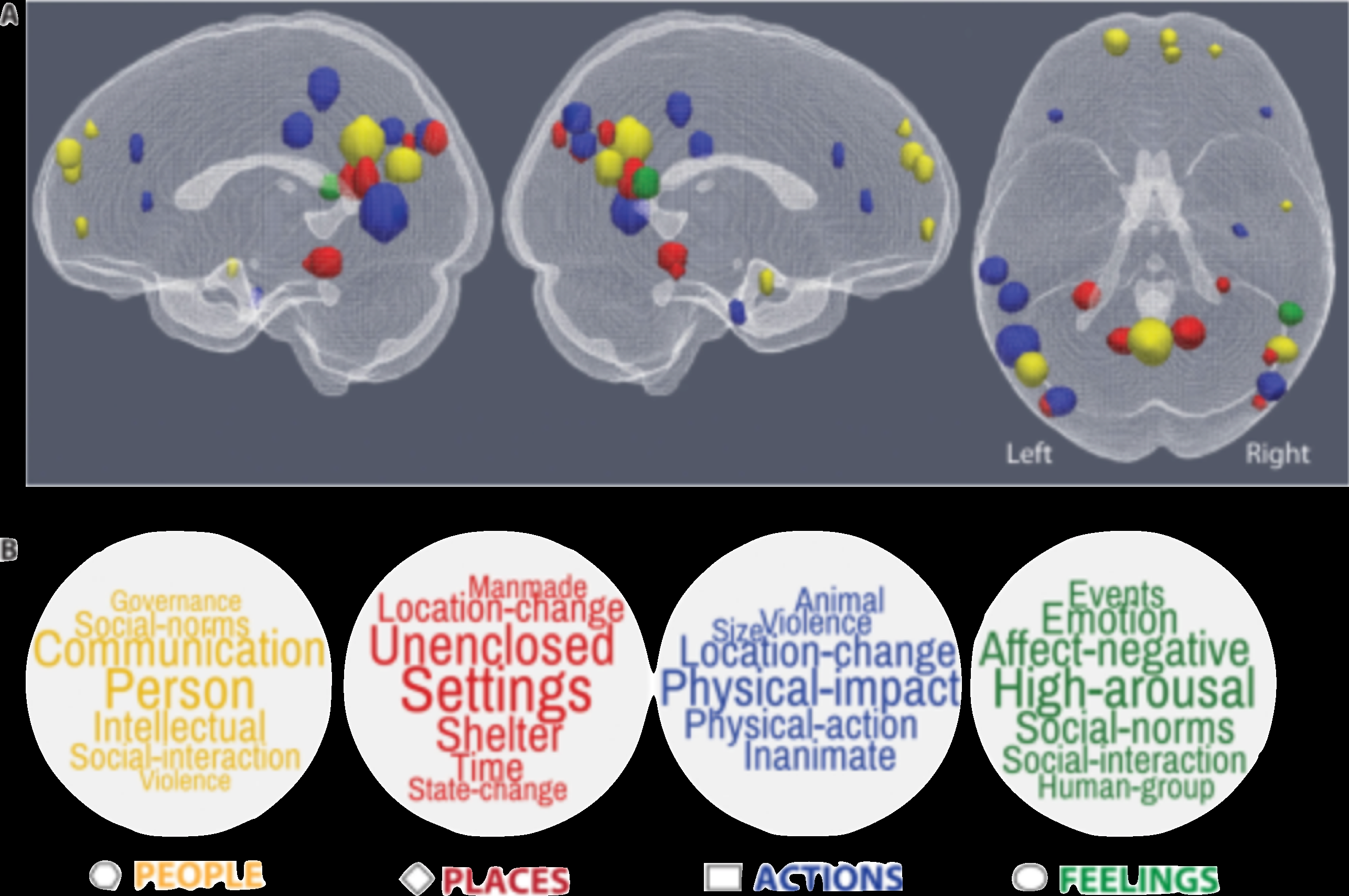
93,94 This discovery led to the idea that the vast majority of concepts central to the human experience can be represented mathematically by a list of 70 numbers. (For the mathematicians, a vector of 70 numbers, or a point in a 70-dimensional space.) Different concepts that are similar, are represented by points in that space that are close to each other. Dissimilar concepts are farther apart. A Doberman is close to a Siberian Husky, but very far from a rose, which in turn is closer to a gardenia.
1.3Memories, Recall & Trauma
Every sensation, feeling (physical, cognitive, and emotional), human participant, social and emotional engagement, timing, and location are part of every memory.
1.3.1What’s Stored in a Memory?
Anyone who has tried to remember something that happened long ago can tell you that their memory storage is imperfect. You don’t remember every detail of everything that’s happened. So what do people’s brains store as memories for later recall? Your memory does not work like a video camera that automatically takes a series of snapshots, each spaced out perfectly in time every 60th of a second. In contrast, our brains have evolved to be massively more efficient and store only those moments most critical for our survival. Think of the brain as an engine that idles, doing little, more-or- less ignoring the world when nothing unexpected or important to survival is happening. But when something critical to survival happens (and this could be good, as in great pair bonding that leads to offspring, or really bad as in the Tiger jumping out from behind the bush to eat you) the engine revs up and starts to store those things so that future you will tend towards repeating the good experiences, and avoiding situations that might harm or kill you. 31,146
1.3.2Four Key Components of Every Memory
There are at least four fundamental aspects of every memory that are stored as an intrinsic part of the learning process (though keep in mind many other aspects are also stored with each memory, but the other aspects vary, depending on what was most noticeable or surprisingly unexpected in the moment): The time it happened, your location where it happened, who was nearby, and whether it was perceived as a beneficial or a harmful memory, and just how good or bad. Other aspects may or may not be stored, depending on how unusual or surprising they were or how closely you happened to be paying attention to specific aspects of the experience.
1.4Attention, Surprise & Novelty
Memory storage is dominated by the novel, unusual, or surprise at the unanticipated. Even unattended aspects that a person wasn’t even explicitly paying attention to might be stored as part of a memory. Recall, on the other hand, can be either driven by focused attention on some notable aspect of a memory, or it can be inadvertently triggered by a new stimulus similar to some aspect of a particularly strongly recorded memory. That stimulus could be external, such as a perfume or
cologne someone was wearing in a past encounter that you smell again today, or it can be internal, as when you remember a particular sweater someone was wearing which then brings into recall the rest of that past memory. 33,138,170 Simply summarized, our brains will mostly store (and be able to later remember) those aspects of an experience which are unusual, unexpected, or surprising, and the more emotionally activated a person was in that moment, the more densely and accurately and comprehensively will those moments be recalled. It’s interesting to note that even in those remembered moments, your brain mechanisms tend to store only the unusual aspects, and not the routine ones.
1.5Emotional Valence Drives Memory Density & Intensity
Memory storage rate (the speed at which new neurons are born and grow, and new neural interconnections are formed) is directly proportional to how emotionally activated the brain is in the moment. Each memory is connected to either the Nucleus Accumbens (positive experience) or the Amygdala (negative) neural circuits. Interestingly, the positive experience and the negative experience circuits have been determined to be oppositional and mutually inhibitory. So when one side is starting to be activated, as in a life-threatening situation that fires up the amygdala and all the downstream fight-or-flight neural circuits and hormonal release, this, in turn inhibits and shuts down those circuits connecting to the amygdala that would neural and hormonally reinforce that behavior. The greater emotional activation in the moment, the stronger and more influential the newly-formed neural circuits become. 15,212 The higher the emotional valence (i.e. the more your limbic system is responding to either a negative stimulus that activates your Amygdala to drive your fight or flight hormones, or conversely when a positive experience revs up your Nucleus Accumbens to drive your dopamine and other reward brain circuits) the faster and more densely your brain lays down new memories. The two critical components that activate memory storage and determine the rate at which new neurons and synaptic connections are created are surprise and emotional activation. 15,212
1.6Memory Storage: Synchrony & Hebbian Learning
A somewhat simplified view of the fundamental memory storage mechanism can be found in the Hippocampus, a tiny horseshoe shaped area of the brain just above the brainstem that sits at the center of both hemispheres of the neo-cortex. Each of the different areas of the broader cortex that all collectively act to represent different information, sensory, concepts, sensations, feelings, etc. are all wired individually and directly to the hippocampus. 61,198,199 When a memorable event occurs that activates our emotional valence and surprises our attention circuits, the hippocampus lays down a new neuron and interconnects every brain circuit that is currently most active in that moment, all to each other, following the Hebbian law that “neurons that fire together” (in synchrony) “wire together.” That includes every notable sensation, thought, feeling, etc. including the neurons representing where and when, as well as whether the amygdala or nucleus Accumbens is activated to capture whether the moment was positive or negative, and how good (or bad).
All of the brain parts that were active at that moment of experience are then forever connected to each other through that new Hippocampal connection neuron. 15,212 Once learned, that memory can be reactivated in full by activating any one aspect of it, which in turn, through that particular memory connection neuron in the hippocampus, transmits that activation proportionately to all the other neurons across the entire cortex that were activated at the moment when that particular event was stored. 61,198,199
One important implication of this rule is that every time a memory is recalled, or a cognitive or physical habit is practiced, the synaptic connections between all the neurons involved in that cognitive process are strengthened and reinforced. The more you think about an event in your past, the more efficient your brain becomes at recalling that event. It takes less energy with every iteration, and less physical and mental effort to recall as a result. This reinforces habits, both mental and physical.
It takes less metabolic energy to do things that you practice as the neural machinery gets more and more efficient with each repetition. 56,100 One aspect of this Hebbian learning and neural metabolic mechanism that is particularly critical to developing newer and improved practices and efficacy in trauma therapy matches what we know about learning, that what you practice thinking becomes habitual thought. If a person practices dwelling on, analyzing, and reliving exclusively negative experiences, as promoted in older talk- therapy-type models, this would only reinforce the neural connections underpinning prior negative experiences and, making it easier and easier for the brain to habitually fall into those negative mental habits.
Importantly, this realization also points to a more definitive theory of why successful EMDR sessions have proven so effective, as well as a whole new set of strategies based on these understandings that promise to radically improve treatment efficacy. 18,81,100
This framework also helps explain why an unsuccessful EMDR session can, at times, lead to a temporary worsening of symptoms. When traumatic memories are recalled in session without proper preparation and/or without in-session efforts to maintain positive framing, activating those memory circuits can lead to undesired looping or inadvertent recall and dwelling upon negative experiences that remain connected only to the Amygdala, actually reinforcing their interconnections and making those negative experiences more neurologically accessible, i.e. easier to recall, and more likely to be triggered by related new stimuli. With only negative review, preparation, or in-session framing, those memory networks remain unintegrated with the nucleus accumbens likely offering little therapeutic effect. 15,212
Reparative neural integration requires the activation of those neural circuits in concert with and to strengthen associative pathways, increasing linkage to affective and motivational circuitry— including reward and salience systems such as the nucleus accumbens.
It is critically important to understand that with poor therapeutic technique, clients may find that trauma responses are triggered more readily, requiring less metabolic energy for activation because the neural pathways have been re-stimulated and reinforced, but not reorganized. 15,212 These new understandings underscores the importance of proper neuro- and trauma-informed approaches when undertaking reprocessing work.
Approaches such as Neural Circuit Integration (NCI), which synthesize multiple trauma-informed modalities, emphasize careful pacing, sufficient resourcing, and the introduction of reparative and regulatory experiences alongside memory activation. By integrating protective, nurturing, and meaning-making elements into the processing sequence, these modifications aim to ensure that when trauma networks are accessed, they are simultaneously linked with neural circuitry that drives positive emotional valence—supporting integration, resolution, and durable healing rather than inadvertent worsening of sensitization.
1.7Overwriting Memories
When a new memory is formed, each one connects to the same cross-brain cortical machinery used to store all other memories. Common machinery across the cortex is used to represent all memories. New memories are added with new neural connections that simply overlay all the connections to older memories, over-writing them. The brain does not specifically erase memories, it overwrites and dilutes related aspects with the addition of new memories. The process of learning a new memory is really a process of adding new and increasingly complex interconnections across brain regions. When new memories create strong new connections, they then, on a relative basis, dilute the relative strength of the older connections to older memories. 56,100 When this happens, the new memory patterns start to over-write the old patterns, and the older memories become more error-ridden with aspects of the new memories corrupting the accuracy and fidelity of the old memories. This is one of the reasons why eye-witness testimony is so unreliable, particularly for older memories of events long-past. People don’t actually remember
exactly what happened with photographic fidelity. What they recall is an admixture of the original stored memory but modified by corrupting inputs from all the subsequently stored memories. 122,123 This also explains why it is possible to discuss novel additions to older memories and implant false aspects of a memory, convincing a person that something happened that didn’t really happen. There are now plenty of examples of court cases where repeated suggestions from biased attorneys have convinced children of things past that never were. Fortunately, this also points to avenues in how to use these phenomena of overwriting old memories to improve therapy. 122,123,146 Therapy, then, is the practice of learning new mental habits that will overwrite, and eventually dilute and dominate the brain’s work offering freedom from old pathological mental habits. Or in terms of the neurophysiology, it is the practice of creating new neural connections from old memory neural circuits to the positive and reward centers of the brain to diminish and counter-balance the influence of those older memory circuit connections to the negative emotional loci of brain activity.
1.8Associative Memories & Energetics
Human memory is intrinsically associative. What this means is simply that all the aspects of a memory are literally interconnected with each other, and activation of one aspect, will activate all the other aspects ASSOCIATED with that experience. With all the sensory, cognitive, and emotional neural circuits of each memory densely interconnected to every aspect of any particular memory, recalling any one aspect of a memory intrinsically triggers the recall of other aspects, led by the most strongly connected memories. I.e. those most emotionally triggering events dominate recall (either positive or negative.)
This is what is called Associative Memory, in the sense that each aspect of a memory is associated to all the other aspects of that memory, and activation of any one aspect will activate the others in turn. We’ve all experienced this when, for example, trying to remember a name…you have the person’s face in your head but can’t remember the name…then you get the first letter, and then the rest of the name comes to mind, and the recall is complete. cortical neurons are all wired together in a complex, densely interconnected network, that is always working. A memory recall is typically triggered by thinking about a single modality, such as "what the apple looked like on the plate yesterday," but in your cortex, all things apple are also stored with synaptic interconnections between them: what it smells like, feels like, how heavy it is, how it decays, or cooks up in a pie, etc.—and through the partial stimulus of the visual aspects, all the other aspects of “apple” are triggered, and strengthened by association. You think of “apple” when you smell one, or see an apple tree, or have one fall on your head. Your brain does this filling-in process from partial information automatically. 5,210,211
An important corollary to this aspect of neural energetics is that it takes metabolic energy, and extra mental effort and discipline to learn and do new things, including developing new healthy mental habits.
This points to a range of pre- and post-session measures that could enhance the effects of therapy, by ensuring proper metabolic fuel is available for a client’s brain to maximize learning. 9,80,133
1.8.1What makes a Traumatic Experience Noteworthy
Recalling that memory storage density and strength is regulated by surprise/novelty and by the level of the brain’s emotional activation, traumatic memories are, by definition, when the brain suffers extreme activation at something that is also, by definition, outside normal experience. The memories stored in moments of trauma are recorded very frequently and with very strong neural coding and synaptic interconnections, and one of the key areas of the brain that is automatically connected to those threatening memories is the Amygdala which in turn activates all the neural and hormonal fight-or-flight systems in the body. This is a direct result of selective pressure in evolving brain circuits that better ensure we remember to avoid such situations in the future. Memories that are stored with stronger interconnections and greater neural activation rates are easier to remember in the future. 99,116
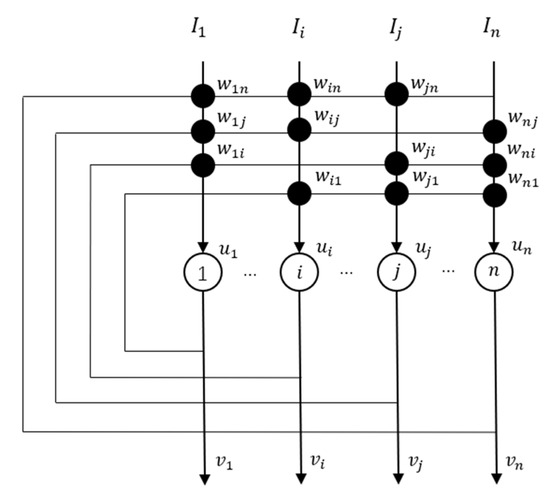
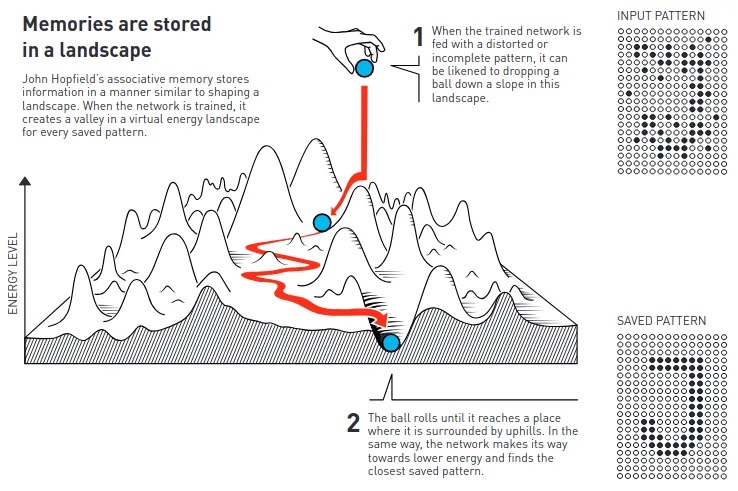
John Hopfield’s associative memory model can be visualized as storing memories in neural activity patters that define valleys in an energy landscape. When the network is prompted with a partial or distorted memory (dropping a metaphorical ball that represents that partial memory state at the beginning of reconnection), the brain then “rolls” through the landscape of stored memory states until the partial memory progressively reactivates more and more of the memory until the brain settles in the nearest valley, representing the fully completed and recalled closest stored memory. This process allows the network to restore incomplete or noisy data by finding the pattern with the lowest energy. Image credit: The Royal Swedish Academy of Sciences, NobelPrize.org.
For those most traumatic memories, the emotional activation can become so powerful in its level and breadth of neural activation, that the system can actually malfunction and store memories with such strength that they can become too easy to activate, to the point where they can be triggered inadvertently when other similar more pedestrian experiences, not so traumatic or strongly encoded, share neural representations with a traumatic memory. It could be the neurons representing a place where trauma occurred, or those representing a person who inflicted the trauma, even when that moment and that person is not threatening in the moment, a unique smell of brake pads and tires from an accident…any other non-threatening experience which shares neural representation with the traumatic memory can initiate the involuntarily activation of the traumatic memory simply by the strength of interconnection to the traumatic one.
The weak interconnections of the pedestrian memory’s neural circuit is overcome by the strong interconnections of the traumatic memory circuit, and a PTSD type event can be triggered involuntarily from seemingly harmless stimulus.
The science also illuminates two possible mechanisms that might explain why people suffering traumatic experiences might suffer memory lapses when trying to recall those memories. Since memory storage rate and density depend on emotional valence, or how hiked-up your emotional response neurons might be, based on the perceived level of threat, greater threats lead to greater neural activation. What this means at a fundamental biophysical level, is that when more strongly activated, the neurons fire action potentials more and more frequently. But it turns out that the neurons in your brain suffer fundamental metabolic limits. Compared to the transistors inside the computers we use, they are glacially slow. A neuron can only fire a signal to another neuron every few milliseconds. After sending a signal, it must recharge itself and re-collect all the neurotransmitter molecules it needs to fire an action potential and then transmit the next signal across its synapse to another neuron. 9,80,133,134
Sometimes, even though the stimulus might get stronger and stronger, a neuron can’t fire any faster when it reaches its physical limit because, driven hard, it has momentarily run out of fuel. The other key limitation is that after firing so many times, a neuron can deplete its local environment of the ions and metabolites it needs to fire, or create a synapse, or convert stem cells into a new neuron. In any of those cases, the memory simply isn’t stored, because having been exhausted by prior activity, the physical building blocks are just not there to support the creation of the physical representation of the memory. With the realization that the traumatic memory storage is the most intensely driven to quickly store as much information as possible and requires the most metabolic energy to accelerate and deepen the neural connection to represent a new experience, those memories that require the most metabolic resources are the most likely to be incomplete or poorly represented or even not stored at all when the metabolic demands of emergency storage overwhelm the local supply of metabolites. The logical result is a possible gap in memory in moments of extreme trauma. 9,80,133
1.9How Time & Causality are Represented
As people live their lives and experience the world around them, their brains automatically and effortlessly store a record, a sequence of memories each as described above, laid down one after the other in sequence. The storage of surprising and emotionally exciting sequences is strong and dense with the most surprising and exciting (either good or bad) aspects being stored with the highest density and fidelity. As they are being recorded in sequence, one of the strongest connections formed in the memory storage is that which connects the temporal coding neurons for one memory, directly to the temporal coding neurons in the subsequent memory. What that interconnection between one neural time code, and the neurons representing the next moment in an experience means is that when one thinks back by focusing their attention on a specific moment in the past, that very recall of a particular moment also begins the activation of the subsequent time code neurons for the next instant, leading directly to the immediate recall of the memory of the next moment, triggering a cascade like a movie of snapshots one memory after the next, and the result is a reimagining of a whole experience one moment in sequence after the next, where each moment’s memory activation also triggers the recall of the next moment’s experience, and so on.
This also explains why particularly traumatic experiences can create very strongly reinforced and capturing memories that once triggered either purposeful or inadvertently by a new stimulus that mimics an aspect of the trauma can start a cascade of re-imagining the whole event, and even repeatedly loop, activating in turn, all of the sensory, body sensation, emotional state, time and place the areas of the cortex as well as those representing high negative emotional valence of a bad experience that should be remembered to advance genetic survival.
This activation in the amygdala then drives the fear and fight/flight response driven by all sensory and cognitive neural apparatus associated that memory connected. Every simple recall of that traumatic memory sequence reinforces those neural connections, including those connections with the amygdala and the fight/flight response that turns off the other thinking parts of the brain and entrapping clients in involuntary memory loops. Again, A simplified, and un-entangled schematic of the cortex highlighting the myriad aspects of memory many memories stored and interconnected across common cortical machinery that use used in concert to represent any and all stored memories.
In mathematical terms, just like reading a sentence in a book creates a neural trajectory of activation patterns, so does the recall of an extended experience. 99,116 We now better understand why and how such re-imagination works to weaken the cognitive entrapment and looping effect of prior trauma. A more complete and updated representation of how abstract ideas and memory sequences are encoded across the entirety of cortex can explain how traumatic memories are densely interconnected-with, and activate all of the sensory, body sensation, emotional state, time and place areas of the cortex as well as those representing high negative emotional valence of a bad experience that should be remembered to advance genetic survival. The activation in the amygdala then drives the fear and fight/flight response driven by all sensory and cognitive neural apparatus associated and connected to that particular traumatic memory.
Every simple recall of that traumatic memory sequence reinforces those neural connections, including those connections with the amygdala and the fight/flight response that turns off the other thinking parts of the brain and entrapping clients in involuntary memory loops.
By adding positive elements, like protective figures, alternative outcomes, and holding positive feelings throughout the re-imaginings, and emphasizing the bodily sensations of comfort, security, safety, satisfaction, and purpose throughout, it is possible to progressively write, with each repetition, new connections from the same neural apparatus formerly only associated with the memories of negative emotional valence experiences (of each sensory modality, sight sound taste, smell, hearing, bodily sensation, people involved, the place and time of occurrence, etc.) and for the first time, write neural connections to the cortical area driving positive emotional valence activities in the nucleus accumbens that leads feelings of positive experiences and rewards behavior with survival benefits. 15,212
With repeated positivity-enhanced re-imaginings, each positive practice reinforces the neural interconnections with the positive reward cortical circuits, and with each addition of a neural connection to the positive experience brain circuits, the influence of the older connections to the amygdala are progressively weakened and step-by-step, progressively lose their ability to dominate the recall process and trap thoughts in the negative loops, offering what is effectively an over- written off-ramp towards positive outcomes.
This effect is further enhanced by the inhibitory effect that positive activation of the nucleus accumbens has on suppressing the amygdala activation when those older traumatic memory circuits are activated. Incidentally, this also offers an explanation why traditional talk therapy, simply dwelling on and considering the negative experience has often demonstrated limited efficacy and can reinforce the trauma-associated neural pathways making activation more likely and problematic in comparison to the newer techniques like EMDR and modification like AF-EMDR and Super Resourcing, Somatic approaches and TIST or IFS. By only recalling and reliving the negative experiences, the neural interconnections to the negative experience neural machinery are simply reinforced, without any clear mechanism to lessen their influence on the fight-flight response. 15,212 These limitations point toward a clear need for therapeutic approaches that work with, rather than against, the brain’s fundamental neural architecture and the neurology of memory and emotional activation and processing.
The foundational modalities described in the following section each address specific aspects of these neural mechanisms—Attachment Theory addresses the relational neural circuitry disrupted by developmental trauma; EMDR leverages bilateral stimulation to facilitate memory re-consolidation and the reprocessing of old trauma patterns to create new more resilient neural circuits along with EMDR modifications to reinforce emotional stabilization; Parts Work addresses the neural basis of structural dissociation; Polyvagal Theory informs autonomic regulation strategies; somatic approaches engage the body’s interoceptive pathways; and mindfulness cultivates the metacognitive capacity for self-regulation. NCI integrates all of these modalities into a unified approach grounded in the neuroscience of distributed memory encoding and neural plasticity. 114,190
1.10Memories Are Not Completely Independent
Because this distributed memory storage mechanism applies each individual region of neurons to represent aspects that apply to many memories. For example, the neurons representing a particular place, or those representing a particular time are connected to all the memories experienced in that place or time. Every bad experience is connected to all the neurons that activate the Amygdala and reinforce the avoidance of that experience. 99,116 Those bad experiences that were the most traumatic are the ones with the strongest connections to the amygdala. When someone asks, “What was your worst experience,” it is simple to turn your attention to activate those bad experience neurons, which in turn activate most strongly, the worst experience, and then subsequently in declining order of those memories associated with weaker and weaker interconnections to the amygdala. 99,116
1.11The Role of the Attention Mechanism
The attention mechanism plays a critical role in memory formation and recall. In memory storage, the brain will primarily store what one is paying attention to in the moment. Importantly, the attention mechanism can either be purposeful, like when one is concentrating intently on something, or accidentally, as when a magician snaps his fingers using a visual and auditory reflex to involuntarily lure one’s attention to the finger motion and the noise, and away from the card he is hiding in his pocket with his other hand. Your automatic reflex to respond to threats involuntarily directs your attention away from what the magician doesn’t want you to remember, and so your brain does not store the sleight-of-hand because it wasn’t paying attention to that hand.
It is also important to note that the attention mechanism can shut down in extremely traumatic experiences, when circuits driving a freeze response are activated and a person stops taking in information, so no memories are stored in that case either. Attention can be hijacked by traumatic memories, leading to involuntary recall patterns. Understanding this mechanism is crucial for developing effective therapeutic interventions. 42,52 With this neuroscience foundation in place—from distributed memory encoding and Hebbian learning to the role of emotional valence and attention in shaping memory—we can now examine why traditional therapeutic approaches have often fallen short. The mechanisms described above reveal specific requirements for effective trauma treatment that many established therapies do not fully address. 18,81,100
Introducing Neural Circuit Integration
Neural Circuit Integration (NCI) is designed for clinicians across therapeutic modalities who want to enhance their existing practice with the latest neuroscience. Rather than replacing what clinicians already do well, NCI offers a neuroscience-informed lens through which to view and strengthen therapeutic work—providing recommendations, strategies, and a structured framework that can be integrated into any evidence-based approach.
The steps outlined in this framework are organized in a logical sequence, but they are intended to be used flexibly. Depending on client readiness, therapeutic goals, and the clinician’s own orientation, elements of NCI can be adapted, reordered, or incorporated as they naturally fit within the clinician’s existing workflow. Some clinicians may use the full framework as presented; others may draw on specific steps or strategies that complement their primary modality. NCI is not a rigid program—it is a set of neuroscience-informed recommendations designed to deepen and enhance the work clinicians are already doing.
NCI is supported by the VitalMe app, which extends the therapeutic process between sessions—reinforcing new neural pathways through guided exercises, personalized meditations, and practice tools. Together, the NCI, supported by the VitalMe app provide a comprehensive, neuroscience-informed framework for case conceptualization and clinical practice.
Foundational Approaches to Trauma Therapy
3.1Phased Trauma Treatment
Judith Herman’s Trauma and Recovery (1992) established the foundational architecture for modern trauma treatment: a three-phase model organized around safety and stabilization, remembrance and mourning, and reconnection. Herman’s central contribution was the recognition that trauma recovery cannot be collapsed into a single therapeutic act—it unfolds in sequence, with each phase requiring its own conditions, pacing, and clinical focus. Stabilization must precede deeper processing, and processing must give way to reintegration into ordinary life and relationship. This phased framework has become the organizing scaffold for nearly every trauma-informed modality that followed, and it remains the consensus structure articulated in international treatment guidelines for complex trauma (Cloitre et al., 2011). NCI honors this architecture: its early steps establish safety and resource the nervous system, its middle steps attend to the wounded parts and the experiences they carry, and its closing steps support integration and re-engagement with a meaningful life.
The phased approach is consistent with what neuroscience reveals about state-dependent learning and neural plasticity. Memory reconsolidation, the formation of new positive circuits, and prefrontal-limbic re-regulation each require a nervous system that is not in sustained sympathetic or dorsal vagal activation—conditions that emerge only when safety and stabilization have been adequately established. Attempting deeper processing before this neurobiological foundation is in place risks reactivating trauma circuits without the conditions necessary for new learning, reinforcing rather than transforming the underlying networks. Where NCI extends Herman’s framework is at the neural level: providing clinicians with the specific mechanisms—cortical activation, nucleus accumbens engagement, multi-sensory stimulation, and memory reconsolidation—by which each phase produces lasting structural change in the brain.
3.2Attachment Theory
Attachment theory, founded by John Bowlby and Mary Ainsworth, provides a critical foundation for understanding how early relational experiences shape an individual’s sense of self, safety, and interpersonal functioning. Secure attachment in childhood fosters emotional regulation, a coherent self-concept, and the capacity for intimacy and trust. In contrast, insecure or disorganized attachment—common in those with complex trauma histories—can lead to internal fragmentation, chronic dysregulation, and relational difficulties. The theory’s primary contribution to trauma therapy is the recognition that restoring a sense of secure internal attachment is essential for healing developmental ruptures, and that the therapeutic relationship itself functions as a reparative attachment experience. Work by Allan Schore and others has extended attachment theory into affect regulation and the development of the self, emphasizing the relational neural circuitry disrupted by developmental trauma and the role of attuned relationship in its repair.
The human attachment system operates through an integrated neural network spanning the anterior cingulate cortex (ACC), ventromedial prefrontal cortex (vmPFC), amygdala, hippocampus, insula, and temporal poles. Feldman (2017) demonstrated that oxytocin and dopamine form critical crosstalk in the striatum, combining motivational vigor with social focus. This neurochemical synchrony enables neural network reorganization around new attachment relationships.
Secure attachment in early life facilitates the development of robust prefrontal-limbic connectivity, enabling effective emotional regulation through top-down modulation of amygdala reactivity. Insecure or disorganized attachment disrupts this connectivity, producing what has been termed cortical dis-connectivity—impaired integration between thinking, planning, and emotional processing regions (Schore, 2015). These early attachment circuits, which develop earlier than cortical systems and maintain deep connections to limbic and autonomic nervous systems, are particularly vulnerable to early attachment disruptions.
When clients visualize nurturing figures providing safety, comfort, and attunement, they activate the same oxytocin-mediated social bonding circuits and ACC-vmPFC networks that would be engaged in actual secure attachment interactions. Repeated multi-modal activation of these circuits during positive reimagining supports the formation of new neural representations of safety and care that can progressively counterbalance the insecure attachment neural circuitry encoded during developmental trauma.
3.3Mindfulness
Mindfulness, brought into clinical practice in the West by Jon Kabat-Zinn and elaborated by many others, is a core element of most trauma-informed therapies. It fosters nonjudgmental awareness of the present moment, supports self-regulation, reduces reactivity, and enhances introspection. Its primary contribution to trauma therapy is that it serves as both a container and a mechanism of change, allowing clients to observe their inner experiences with curiosity and compassion without becoming overwhelmed or fully identified with them. Mindfulness provides the metacognitive capacity for self-regulation that underpins trauma processing across modalities—whether as the foundational observing stance in parts work, the titrating awareness in somatic tracking, or the dual-attention anchor in trauma reprocessing.
Mindfulness meditation produces measurable changes in brain structure and function across multiple networks relevant to trauma processing. The default mode network (DMN)—involved in self-referential thinking, rumination, and mind-wandering—shows reduced activity during meditation and altered resting-state connectivity patterns with sustained practice. For trauma survivors, who often experience intrusive self-referential rumination, this modulation of DMN activity offers a neural mechanism for reducing the automatic cycling through trauma-related thoughts.
Yi-Yuan Tang’s research demonstrated that even brief mindfulness training (as few as 11 hours) produces measurable changes in the anterior cingulate cortex (ACC), increasing both ACC activity and structural white matter changes in surrounding fibers. The ACC plays a central role in attention regulation, conflict monitoring, and error detection—functions essential for the metacognitive awareness that allows trauma survivors to notice triggering stimuli without becoming captured by automatic trauma responses.
Mindfulness training also produces significant changes in the insula cortex. Studies of populations undergoing mindfulness-based training show attenuated right anterior insula and ACC responses during aversive interoceptive challenges, suggesting that mindfulness enhances the capacity to process difficult bodily sensations without overwhelm.
Perhaps most important, mindfulness consistently improves ventromedial prefrontal cortex–amygdala and nucleus accumbens functional connectivity—the central emotion regulation pathway disrupted in PTSD. By strengthening this top-down regulatory capacity, mindfulness enhances the brain’s ability to modulate amygdala reactivity to threatening stimuli, engaging the reciprocal inhibition mechanism through which positive reimagining can progressively counterbalance trauma-activated fear responses.
3.4Polyvagal Theory, Somatic Interventions, and the Window of Tolerance
Polyvagal Theory, developed by Stephen Porges, deepens our understanding of trauma by explaining how the autonomic nervous system responds to threat. The model describes three primary states—social engagement (ventral vagal), mobilization (sympathetic), and immobilization (dorsal vagal)—and demonstrates that trauma often traps individuals in sympathetic or dorsal states, impairing connection and self-regulation. Its central contribution is a physiological map of safety and threat that gives clinicians a framework for recognizing and shifting autonomic states through co-regulation, vagal toning, and cues of safety.
The Window of Tolerance, developed by Daniel Siegel, describes the optimal arousal zone in which individuals can engage in reflective thinking, emotional processing, and adaptive functioning. Trauma survivors often oscillate between hyper-arousal (fight/flight) and hypo-arousal (freeze/collapse), making therapeutic work difficult without adequate regulation. Siegel’s primary contribution is the clinical framework for titrating therapeutic work within bearable activation—an organizing principle now embedded across trauma-informed modalities.
Somatic approaches—including Sensorimotor Psychotherapy (Pat Ogden), Somatic Experiencing (Peter Levine), and the body-centered trauma work articulated by Bessel van der Kolk—recognize that trauma is stored in the body. These approaches focus on restoring bodily awareness and resolving trauma-related activation through movement, posture, breath, and autonomic regulation. Their main contribution is the clinical recovery of the body as a site of both trauma and healing: engaging interoception, completing thwarted defensive responses, and using somatic markers (breath, muscle tone, temperature, autonomic settling) as indicators of processing and integration.
Taken together, Polyvagal Theory, the Window of Tolerance, and somatic interventions provide the bottom-up foundation of trauma work—ensuring that therapeutic processing occurs within a physiologically regulated state and that the body’s wisdom is engaged as a partner in healing.
Polyvagal-informed approaches offer quantifiable biomarkers for tracking therapeutic progress. Respiratory sinus arrhythmia (RSA)—the periodic variation in heart rate synchronous with breathing—serves as a measurable index of cardiac vagal tone via ventral vagal pathways. PTSD patients consistently demonstrate decreased heart rate variability, reflecting autonomic states biased toward sympathetic mobilization with diminished vagal regulatory capacity. As therapeutic work progresses, improvements in HRV provide objective evidence of nervous system reorganization.
Severe dissociative responses involve activation of periaqueductal gray (PAG) circuits associated with immobility and tonic immobility (freeze) responses—the most primitive defensive response in the mammalian repertoire, corresponding to dorsal vagal shutdown. When PAG circuits dominate, clients experience depersonalization, derealization, and emotional numbing—the subjective correlates of defensive immobilization.
The neuroscience of body-based trauma processing has been substantially advanced by research on interoception—the nervous system’s capacity to sense, interpret, and integrate signals from within the body. The insular cortex serves as the primary cortical hub for interoceptive processing. The posterior insula receives primary visceral and bodily signals, while the anterior insula integrates these with higher cognitive and emotional functions, producing the subjective sense of how the body feels in the present moment (Craig, 2009). Van der Kolk’s research demonstrates that trauma fundamentally alters insula function, rendering traumatized individuals less able to sense their own internal states—a disruption that impairs both emotional regulation and the capacity for pleasure and engagement.
Somatic Experiencing works through interoceptive and premotor cortical pathways. Payne, Levine, and Crane-Godreau (2015) demonstrated that SE points clients toward non-verbal experiences of internal bodily sensation, proprioception, and kinesthetic awareness mediated by the insular cortex, anterior cingulate gyrus, premotor cortex, and parietal cortex. Trauma disrupts the completion of defensive motor responses—the freeze response represents an incomplete fight-or-flight sequence—and SE facilitates the completion of these responses to resolve the physiological imprint of trauma.
Techniques that promote ventral vagal engagement—grounding, somatic tracking, imagined safety, connection, and compassion—prepare the brain for improved neuroplasticity, neurogenesis, and synaptic formation. Regulated autonomic states create the neurobiological conditions under which new positive circuits can be laid down and strengthened, leveraging the oppositional circuitry between the amygdala and the nucleus accumbens described in Section 1.
3.5EMDR
EMDR, developed by Francine Shapiro, is a widely validated treatment for trauma that utilizes bilateral stimulation (e.g., eye movements) to reprocess disturbing memories. It is grounded in the Adaptive Information Processing (AIP) model, which proposes that psychological distress arises when traumatic or overwhelming experiences are inadequately processed and stored in a maladaptive memory network. The EMDR process allows a memory to integrate with adaptive information, leading to reduced emotional distress, shifts in negative beliefs, and the spontaneous emergence of more adaptive emotions, sensations, and cognitions.
EMDR’s primary contributions to trauma therapy are several: it established the clinical efficacy of a protocolized, neurobiologically-grounded memory reprocessing approach; it introduced bilateral stimulation as a means of engaging working memory and facilitating reconsolidation; and its three-pronged structure—addressing past memories, present triggers, and future templates—provides a comprehensive framework for trauma resolution. While highly effective for single-incident trauma, EMDR in its standard form is often insufficient for clients with complex or C-PTSD from repeated experiences, who require more preparatory work and attention to attachment and the entire timeline of traumatic experiences.
The neuroscience of memory reconsolidation provides explanatory support for EMDR. Research following Nader, Schafe, and LeDoux’s 2000 discovery demonstrated that reactivated memories require new protein synthesis for restabilization, entering a temporarily labile state during which they can be modified. A critical requirement for triggering this reconsolidation window is prediction error—a mismatch between what the memory predicts and what is currently experienced. EMDR’s reactivation of the trauma memory within a safe therapeutic context naturally generates this mismatch, opening the reconsolidation window for therapeutic modification.
Bilateral stimulation also appears to tax working memory in ways that reduce the vividness and emotional charge of recalled trauma. Engaging visual, auditory, and somatosensory systems simultaneously distributes cognitive load across neural systems, supporting the desensitization of the memory’s emotional intensity.
The broader neural architecture of memory—distributed across the entire cortex, densely interconnected through the hippocampus, and anchored to emotional valence via the amygdala and nucleus accumbens—explains why EMDR works and where it reaches its limits. Reactivating a trauma memory without accompanying positive-valence activation can strengthen the trauma circuitry it was meant to resolve. Effective reprocessing requires that the reactivated memory be linked to new, adaptive information with strong connections to positive emotional and motivational systems.
3.6Attachment-Focused Modifications of EMDR: Parnell, Schmidt, Teal
A family of attachment-focused modifications to EMDR emerged to address the needs of clients with complex trauma, developmental trauma, and attachment wounding—populations for whom standard EMDR protocols often proved insufficient.
Laurel Parnell developed Attachment-Focused EMDR (AF-EMDR), which emphasizes strong resourcing through imaginal attachment figures to support stabilization and preparation for processing, and the use of imaginal interweaves to facilitate adaptive information processing. Parnell’s principal contribution is the systematic integration of imaginal nurturing, protective, and wise figures into the EMDR protocol—treating the internalization of secure attachment as essential groundwork and as an active ingredient in reprocessing.
Shirley Jean Schmidt advanced attachment-oriented EMDR through the Developmental Needs Meeting Strategy (DNMS), which integrates EMDR with ego state work and nurturing internal figures to address unmet developmental needs. DNMS’s contribution is a structured method for identifying the developmental ages at which needs went unmet and for offering those specific unmet needs to the parts that still hold them, with EMDR facilitating integration.
Alison Teal developed Super-Resourcing (SR), which integrates EMDR with parts-focused healing to facilitate corrective emotional experiences. SR leverages imagination to address unmet developmental needs, fostering resilience. It expands upon traditional EMDR by prioritizing positive reparative experiences and integrating parts work: clients actively create imaginal experiences that reflect what they needed or wanted to receive, offering parts experiences of safety, care, connection, and support. Therapeutic focus is then directed toward the positive emotions, sensations, and cognitions that emerge from these imagined reparative experiences. Teal’s main contribution is the explicit therapeutic use of imaginal reparative experiences and the emphasis on strengthening positive states rather than desensitizing negative ones.
Together, these three modifications share a common clinical insight: for complex and developmental trauma, preparation, resourcing, and the creation of positive, corrective internal experiences are central to healing—not peripheral to exposure.
These attachment-focused modifications pioneered a clinical approach that aligns closely with the neuroscience of how new positive neural circuits can be created and how they counterbalance trauma circuits.
By adding positive elements—protective figures, alternative outcomes, and positive feelings held throughout re-imaginings—and emphasizing bodily sensations of comfort, security, safety, satisfaction, and purpose, it is possible to progressively write, with each repetition, new connections from the neural apparatus formerly associated only with memories of negative emotional valence to the cortical area driving positive emotional valence activities in the nucleus accumbens.
With repeated positivity-enhanced re-imaginings, each positive practice reinforces the neural interconnections with positive reward cortical circuits. With each added connection to the positive experience brain circuits, the influence of the older connections to the amygdala is progressively weakened. Step-by-step, these older connections lose their ability to dominate the recall process and trap thoughts in negative loops—effectively an over-written off-ramp toward positive outcomes. This effect is further enhanced by the inhibitory effect that nucleus accumbens activation has on the amygdala when older traumatic memory circuits are engaged.
Viewed through the lens of current neuroscience, the clinical intuitions of Parnell, Schmidt, and Teal were early operational discoveries of a core neural mechanism of healing: creating positive, reparative circuits densely connected to the nucleus accumbens that progressively outcompete amygdala-linked trauma circuits.
3.7Ego State and Parts Work: TIST and IFS
Clients with Complex PTSD often present with symptoms of structural dissociation—disconnected parts of the personality that hold trauma, protection, or adaptive functioning. Parts-based approaches treat these fragmented self-states as distinct internal agents and work to restore internal communication, compassion, and integration.
Trauma-Informed Stabilization Treatment (TIST), developed by Janina Fisher and grounded in the structural dissociation theory of van der Hart, Nijenhuis, and Steele, emphasizes the need to work with these parts gently and respectfully. TIST integrates psychoeducation, parts mapping, and somatic mindfulness to help clients stabilize and develop self-compassion for all parts, relying on the “going on with normal life” part as the guide and caregiver of the wounded parts. Its main contribution is a trauma-specific parts framework that centers stabilization and self-compassion before any deeper processing, and that explicitly links parts to the neurobiology of defense.
Internal Family Systems (IFS), developed by Richard Schwartz, offers a comprehensive framework for parts work by facilitating a relationship between the Self—a wise, compassionate inner leader—and various internal parts (commonly organized as Exiles, Managers, and Firefighters). While not explicitly based on structural dissociation, IFS aligns with the goals of TIST in creating internal harmony and integration. Its primary contribution is the concept of the Self as the natural healer of parts and a systematic method for unburdening exiles and renegotiating the roles of protectors.
Together, TIST and IFS provide complementary routes to the same therapeutic aim: respecting the protective and adaptive functions of parts, acknowledging the wounds they carry, and supporting the development of an internal relationship in which wounded parts receive the care and integration they have long been waiting for.
The structural dissociation model’s distinction between “going on with normal life” parts and “wounded parts” finds support in neuroimaging studies showing distinct neural signatures for different self-states. Research by Schlumpf et al. (2014) demonstrated that dissociative identity disorder patients show different neural activation patterns across identity states, with trauma-holding states showing increased limbic activation and avoidant states showing decreased limbic engagement. This validates the clinical experience of distinct parts with different emotional, somatic, and cognitive characteristics.
Parts can be mapped onto identifiable neural systems. A mindful, observing presence corresponds to activation of medial prefrontal and insular regions associated with metacognitive monitoring and interoceptive awareness. The aspect of self that manages daily functioning and maintains present-time orientation is associated with activity in the default mode network, which supports autobiographical self-reference, coherence of identity, and future-oriented planning. Protector parts are frequently mediated by rapid subcortical threat circuits, enabling automatic and reflexive responses outside of conscious cortical appraisal. Wounded parts reflect distinct neural assemblies associated with autobiographical memory and emotional processing that differ from present-moment self-representation—encoding the unprocessed sensory, emotional, and somatic material of the trauma and experiencing triggers as if the threat were still present.
Dissociation itself has identifiable neural correlates. Functional neuroimaging studies show that dissociative states involve altered connectivity between cortical regions responsible for conscious processing and limbic structures involved in emotional experience. Increased activation in medial prefrontal cortex coupled with decreased amygdala activity characterizes dissociative detachment—a pattern suggesting top-down inhibition of emotional processing. The default mode network itself shows altered connectivity patterns in dissociative disorders, mapping onto the clinical experience of identity fragmentation and altered self-states.
Together, these findings provide a neurobiological foundation for parts-based conceptualizations and demonstrate that the fragmentation clinicians observe is not metaphorical but reflects measurable patterns in brain network connectivity.
The NCI Framework
Neural Circuit Integration model refines, extends, and unifies the most effective approaches to trauma therapy in a single comprehensive framework as supported by the latest neuroscience.
Neural Circuit Integration is a framework of neuroscience-based recommendations, strategies, and extensions that translate the neuroscience of Section 1 into specific in-session and between-session enhancements clinicians can layer onto whatever trauma-informed approach they already use. NCI sits alongside—and draws from—EMDR, Attachment-Focused EMDR, Super-Resourcing, DNMS, TIST, IFS, Polyvagal-informed work, somatic approaches, and mindfulness, offering a shared neuroscience lens and a set of concrete enhancements that deepen the work each of these modalities already does well.
4.1NCI as a Framework That Builds on Existing Modalities
NCI is designed to fit into and deepen existing clinical work.
For EMDR-trained clinicians, NCI offers: mindful presence as the observing platform that supports dual attention during processing; adapted history-taking that reduces premature activation of trauma networks and emphasizes current symptoms, strengths, and adaptive capacities; pre-session neuroplasticity practices that strengthen ventral vagal states before processing; attachment-focused resourcing drawn from Parnell before any trauma reprocessing; extended positive-resolution work drawn from Teal’s Super-Resourcing with NCI prompting cues to deepen cortical engagement; post-session reinforcement on the VitalMe app to stabilize newly formed pathways; and the NCI Timeline Model, which links target memories to associated developmental experiences organized around similar emotions, beliefs, and somatic states. After installation of reparative imagery and adaptive resolution, clinicians extend these corrective experiences across the life timeline—allowing adaptive cognitions, emotions, and embodied safety states to generalize across clustered trauma imprints rather than remaining isolated to a single event. NCI also extends EMDR’s future templating through the Manifestation Phase, supported in the app.
For parts-work clinicians using TIST or IFS, NCI adds: imagined reparative experiences designed to meet unmet developmental, relational, and emotional needs held by wounded parts; structured NCI prompting to activate higher-order cortical involvement during parts work—engaging beliefs, meanings, sensations, relational dynamics, and environmental context simultaneously; app-based practices that cultivate the observing or noticing part, strengthening the metacognitive awareness that supports dual attention and the capacity to witness wounded material without overwhelm; pre-session practices that promote positive affective and physiological states before parts work; bilateral and multi-sensory stimulation during imagined reparative moments to deepen encoding across multiple sensory processing channels; timeline integration to extend reparative experiences across associated developmental stages; post-session reinforcement to stabilize and consolidate newly formed adaptive circuits between sessions; and manifestation-oriented protocols that support the Life Navigator in orienting toward future growth, purpose, and adaptive life expression.
For somatic clinicians working from Ogden, Levine, or van der Kolk, NCI provides complementary neural activation strategies that deepen and expand body-based trauma processing: combining bottom-up somatic tracking with top-down, multi-dimensional imagery to engage both subcortical and cortical networks; pre- and post-session neuroplasticity practices that promote regulation, safety, and positive affective states that enhance receptivity to somatic processing; positive somatic anchoring paired with multi-modal stimulation to strengthen embodied experiences of safety, connection, and support; embodied reimagining that invites clients to notice posture, movement impulses, gestures, and shifts in physical orientation within imagined scenarios; multi-sensory engagement of bilateral tones, tactile tapping, and visual tracking while adaptive body states are activated; somatic markers (breath, muscle tone, temperature, autonomic settling) as real-time feedback for stabilization, completion, and adaptive resolution; and app-based somatic reinforcement exercises that stabilize and generalize embodied safety states between sessions.
For polyvagal-informed and somatic clinicians, NCI offers: co-regulation and ventral vagal engagement as the physiological foundation for neural integration work; amplification of ventral vagal states through positive activation paired with multi-sensory stimulation, deepening encoding of safety and connection across autonomic and cortical networks; mindful awareness of regulated states as preparatory groundwork for reparative reimagining; and ongoing autonomic monitoring during reimagining to ensure processing remains within the Window of Tolerance. Grounding and nervous-system regulation practices are used at the opening of each session to cultivate ventral vagal engagement, because the social engagement system is the brain’s optimal state for learning, relational receptivity, and memory reconsolidation. Examples supported in the VitalMe app include 4-4-8 breathing (inhale for 4, hold for 4, exhale for 8), box breathing, extended-exhale breathing, grounding-cord visualization, toning and humming to activate the vagus nerve, and gentle self-holding or hand-on-heart to engage the ventral vagal system. These practices are not merely calming techniques—they intentionally cultivate the neurobiological safety required for neuroplastic change, and are available to clients between sessions through the app to extend regulation practice into daily life.
Across modalities, NCI also brings a specific orientation to intake and history-taking. The neuroscience of Section 1 is direct: each detailed retelling of a traumatic memory reactivates the neural circuits associated with it—including the amygdala-driven fear and threat-detection pathways that hold the trauma in place—and each activation requires less metabolic energy the next time, making the pathway more efficient and more easily triggered. Extensive trauma-history taking at intake risks rehearsing and consolidating the pain rather than resolving it. NCI suggests approaching intake with care around detailed trauma narratives—listening with attunement when the client shares, while orienting the intake around current symptoms, strengths, supportive relationships, and the client’s own hopes for therapy. Events that need processing surface organically through the trace-back technique, parts work, and the body’s signals; a comprehensive trauma inventory is not a prerequisite for beginning the work. Accessible psychoeducation about how trauma is stored in amygdala-linked circuits and how healing builds competing nucleus accumbens–linked circuits is also offered as part of intake.
Throughout, the framework preserves attribution. Its phased structure honors Judith Herman’s foundational three-stage model of recovery. NCI’s resourcing and imaginal repair build on the work of Parnell, Teal, and Schmidt. Its parts work is informed by Fisher and Schwartz. Its regulation foundations draw from Porges, Siegel, Dana, and Ogden. Its memory reprocessing is rooted in Shapiro. Its somatic work is grounded in Ogden, Levine, and van der Kolk. Its mindfulness acknowledges Kabat-Zinn and the broader contemplative tradition.
4.2Mindful Awareness
Beyond its foundational role across trauma-informed therapies (Section 3.3), Mindful Awareness is cultivated as a specific in-session practice in NCI. The clinician guides the client to access the observing presence within that notices—inviting awareness of the differentiation between the feelings, thoughts, or experiences the client is having and the awareness that knows they are having those thoughts, feelings, and experiences. From this place, the client can begin to notice the different neural circuits and states active within their experience—the integrative and adaptive circuits of the Life Navigator, the survival-based protective responses, the trauma-encoded networks, and the deeper qualities of the Wise Self. Clients often describe this shift as a felt sense of stepping back from the noise—a moment of quiet clarity where thoughts and feelings are still present but no longer overwhelming.
Why this matters neurologically: developing Awareness is not only a mindfulness practice—it simultaneously activates deep cognitive processing circuits that have a direct inhibitory effect on threat-based activation. When attention is deliberately directed to present-moment experience, it engages the frontoparietal control network, dorsolateral prefrontal cortex, and anterior cingulate cortex—the brain’s analytical and executive processing systems. This activation has two important inhibitory consequences: it suppresses default mode network activity, reducing the ruminative and self-referential processing associated with depression and anxiety; and it exerts top-down inhibitory control over the amygdala, reducing its reactivity to threat cues. Medial prefrontal cortex input to the amygdala functions as an inhibitory signal, dampening fear circuit activation and reducing the automatic emotional reactivity that keeps trauma responses entrenched. Mindfulness attention does not simply calm the nervous system—it structurally competes with and progressively weakens amygdala-linked trauma circuitry by recruiting the same cortical systems that trauma has worked to suppress. Over time, this builds the neural infrastructure—stronger prefrontal regulation, reduced amygdala reactivity, greater insular awareness—that makes all subsequent therapeutic processing safer and more effective.
What the VitalMe app offers: guided Awareness exercises that clients can practice between sessions to deepen the observing capacity, with optional MSS elements to strengthen the neural circuitry of mindful attention.
4.3The Life Navigator
Once Awareness is established, the client can turn attention toward the Life Navigator—the aspect of self that integrates cortical resources and inhabits daily life.
The Life Navigator — development of the integrative, adaptive self that inhabits present-day life. This draws from Fisher’s “going on with normal life” part and Schwartz’s concept of Self while anchoring them in the neuroscience of cortically-mediated executive function. The Life Navigator operates through the prefrontal cortex and its associated networks—the capacity for appraisal, flexible planning, and conscious choice that is distinct from the automatic, subcortical survival responses of the limbic system. Helping clients recognize and inhabit the Life Navigator is itself a corrective experience.
Neuroscience of the Life Navigator. The Life Navigator reflects the integrated activity of higher cortical networks—particularly the dorsolateral and medial prefrontal cortex, the anterior cingulate cortex, and the default mode network in its integrative (rather than ruminative) mode. These systems support appraisal, flexible goal-directed behavior, autobiographical self-reference, future-oriented planning, and the coherence of identity across time. This is categorically different from the rapid, reflexive responses of subcortical threat circuits, which activate automatically and bypass cortical processing. When clients are guided to identify, name, and embody Life Navigator qualities, the repeated activation of these cortical networks strengthens prefrontal–limbic regulatory pathways—the top-down connections through which medial PFC input dampens amygdala reactivity. Each activation is a Hebbian event: the circuits that represent capability, wisdom, relational competence, and adaptive action become more densely interconnected and more easily accessible. Reinforcement with multi-sensory stimulation broadens the cortical surface recruited during this encoding, deepening the neural representation of the Life Navigator as a stable, available state.
Clinicians are encouraged to invite a brainstorming process with the client to identify Life Navigator qualities and attributes: patience, kindness, discernment, confidence, intuition, resilience, determination, creativity, courage, resourcefulness; talents, skills, interests, and hobbies; positive relationships, friendships, and meaningful connections; family roles and commitments; professional accomplishments; responsibilities managed with care; creative pursuits and areas of learning; moments of humor, joy, and lightness; and specific examples of completed life tasks that demonstrate Life Navigator capabilities. The list is read back to the client and reinforced with MSS—feeling the length of the spine and core can help with embodiment. The Life Navigator then serves as the internal guide and secure base for all neural circuits, with compassionate Awareness as the one who notices all of them. Life Navigator qualities are recorded in the VitalMe app, which generates a personalized Life Navigator meditation incorporating those qualities.
4.4Multi-Sensory Stimulation (MSS): Extending Bilateral Stimulation
NCI incorporates Multi-Sensory Stimulation (MSS) throughout the framework as a way to deepen neural encoding during therapeutic moments. MSS builds on the foundation of Bilateral Stimulation (BLS), which originated in EMDR.
The original theoretical model for BLS—alternating hemispheric activation—is now considered outdated by current neuroscience. The brain does not function as two distinct hemispheres operating independently; rather, the full cortex is involved in all neural processing, with distributed networks spanning both hemispheres working together as integrated circuits (Section 1.1). BLS remains a useful clinical tool, not because it activates one hemisphere at a time, but because it adds sensory stimulation that activates neurons and supports the conditions for new learning and encoding.
MSS extends this principle by engaging multiple sensory channels simultaneously. With the associative memory aspect of multi-modality memory, traumatic experiences are densely stored neural cascades that include recordings from all of the client’s senses and bodily feelings, emotions, and so on—each exploits the broad activation of the entire cortex. So therapies that involve higher levels of neural activation across more sensory modalities, and that connect more aspects of the activating memories to positive emotional neural circuits, offer more efficacious neural overwriting. The efficacy is roughly proportional to the total brain volume dedicated to that sensory modality: vision, which dominates the cortical machinery, is the most powerful; then hearing, then smell, then taste, then somatosensory input.
Complex, time-varying stimulation activates more neural circuitry than simple static stimulation. Simple static imagery—like a stationary exam room or a fixed Zoom frame—offers little visual cortex activation. Natural scenery with constant motion across spatial and temporal scales produces the greatest activation: a forest with tree branches and leaves in motion, or a coastal scene with complex waves. The same principle holds for auditory stimulation: complex binaural soundscapes with changing tone, rhythm, and spatial qualities activate more auditory neurons than simple tones. Susurration—rain, flowing water, wind, varying white noise—also engages the auditory cortex effectively.
What the VitalMe app offers for MSS: guided MSS sessions pair complex visual stimulation (walking along a forest path, watching a kaleidoscope, moving through natural coastal or woodland scenery) with layered auditory input (music, nature sounds, tonal patterns, binaural elements) that change over time. Both BLS and MSS options are available, so clinicians and clients can choose what works best. MSS is designed to be woven into resourcing, imaginal repair, parts integration, timeline work, and future visualization—any moment in the therapeutic process where the goal is to strengthen a new positive circuit.
4.5The NCI Noticing Prompts: A Framework for Maximum Cortical Engagement
A core NCI innovation is a structured set of Noticing Prompts designed to activate the broadest possible distributed cortical network during positive reimagining, resourcing, parts work, and future visualization. The principle is grounded in Section 1’s neuroscience: distributed memory re-encoding requires distributed re-activation. When traumatic memories are stored, they encode across multiple cortical systems simultaneously—creating a dense network of associations across visual, auditory, somatosensory, temporal, social, and emotional processing regions. To effectively create competing positive memory traces, therapeutic reimagining must similarly activate these broadly distributed networks.
Each prompt category targets specific cortical regions and neural systems:
Safety & Relief — amygdala down-regulation; ventral vagal activation; shift from sympathetic/dorsal dominance toward ventral vagal social engagement
Supportive Presence — attachment circuitry (ACC, vmPFC); oxytocin-mediated social bonding; mirror neuron system; temporoparietal junction (TPJ)
Sensory Pleasantness — multi-modal cortical activation across sight (visual cortex, ~35% of cortical volume), sound (auditory cortex, superior temporal regions), smell (piriform cortex, orbitofrontal cortex—with direct amygdala connections for emotional memory reconsolidation), taste (gustatory cortex, orbitofrontal cortex, insular cortex), and touch/sensation (somatosensory cortex, insular cortex for interoception)
Emotional Shifts — nucleus accumbens, ventral striatum, dopaminergic reward pathways; reciprocal suppression of amygdala fear response
The Body’s Response — full interoceptive network: brainstem regulatory nuclei → insula → prefrontal cortex
Being Valued & Protected — attachment circuitry paired with reward systems (ACC, vmPFC, oxytocin and dopamine systems, medial PFC, TPJ)
Belonging & Connection — social-relational circuitry (medial PFC, TPJ, mirror neuron system, oxytocin-mediated bonding networks)
Meaning & Awe — salience network; default mode network in integrative (rather than ruminative) mode; meaning-making and narrative coherence
Choice, Agency & Empowerment — dorsolateral prefrontal cortex (executive function), premotor cortex (action planning), nucleus accumbens (motivational drive)
Time & Integration — hippocampal time cells and temporal coding neurons that organize memory sequence, used here to assert “then vs. now” and disrupt traumatic looping
Reward & Wanting-to-Keep — nucleus accumbens consolidation; Hebbian reinforcement through each moment of “wanting more”
Closing Integration — full cortical summary: simultaneously activating visual, auditory, somatosensory, olfactory, emotional, cognitive, temporal, and relational representations for maximum Hebbian consolidation across the entire distributed memory network
The more cortical regions simultaneously activated, the more effectively new positive neural connections can overwrite and dilute older trauma-associated patterns. The prompts are written to be used flexibly within any modality and are included in the VitalMe app as a reference guide for clinicians.
4.6Resourcing as Active Neural Rewiring
NCI’s resourcing work is directly informed by Laurel Parnell’s Attachment-Focused EMDR and Alison Teal’s Super-Resourcing.
Parnell introduced the clinical practice of offering developmental repair to the younger wounded self as a stand-alone therapeutic process—returning to the moment of unmet need and providing, through imagination and the therapeutic relationship, the nurturing, protective, or wise figure that should have been there. Separately, she developed the resource interweave and other interweaves as clinical moves applied during EMDR processing, bringing imaginal figures, alternative missing experiences, and adaptive information directly into the reprocessing field. These two contributions—developmental repair as a stand-alone practice, and interweaves as active ingredients during processing—together expanded what resourcing could accomplish in trauma therapy.
Alison Teal’s Super-Resourcing extended this work by integrating Janina Fisher’s TIST parts work. Teal’s contribution was to locate and work with specific wounded parts of the self, to offer each part the reimagined reparative experience it needed but never received, and to focus therapeutic attention on the positive emotions, sensations, and cognitions that emerged from those imagined experiences. Equally central to super-resourcing is the clinician’s relational stance: the work is delivered with deliberate warmth, empathic attunement, and embodied presence—facial expression, vocal prosody, eye contact, breath, and felt resonance all serving as co-regulating cues that invite the client’s nervous system into the ventral vagal state of social engagement described by Polyvagal Theory (Section 3.4). This relational warmth is not incidental; it is itself a therapeutic ingredient—the autonomic ground that makes new attachment encoding, memory reconsolidation, and the felt reality of the reparative experience possible. Together, these elements establish the positive state, held within an attuned therapeutic relationship, as an active therapeutic ingredient in its own right.
NCI builds on both contributions by adding structured multi-sensory cortical prompting to each reparative moment. Where Parnell and Teal establish the clinical moves—developmental repair for the younger wounded self, interweaves during processing, and reimagined reparative experience for the specific part—NCI’s contribution is to maximize the cortical breadth and depth of each experience, activating as much of the distributed cortical network as possible during each repair. When clients vividly imagine nurturing, protective, and supportive figures, they activate oxytocin-mediated social bonding circuits and ACC–vmPFC networks—the same circuits engaged in actual secure attachment interactions. With NCI’s Noticing Prompts applied across visual, auditory, somatosensory, interoceptive, relational, temporal, emotional, and meaning-making domains simultaneously, the reparative experience is encoded across the broadest possible cortical surface, driving activation toward nucleus accumbens–linked positive circuitry and creating new neural representations of safety, support, and belonging that progressively compete with and counterbalance the insecure attachment and threat-based circuitry encoded during trauma.
NCI also offers the option of Multi-Sensory Stimulation (MSS) and Bilateral Stimulation (BLS) throughout resourcing to enhance neuroplasticity. Pairing each reparative moment with MSS or BLS recruits additional sensory cortex, adds sensory novelty that supports new encoding, and deepens the Hebbian reinforcement of the new positive circuitry—making the neural change more durable and accessible between sessions.
NCI offers several interlocking and mutually-reinforcing forms of resourcing:
The Resource Team — protector, nurturer, wise figure, healer, champion, playful figure, peaceful place, compassionate figures (building on Parnell and Teal). Each figure is explored through a full NCI prompt set that engages sight, sound, touch, body sensation, emotion, belief, belonging, and awe—then reinforced with MSS.
The Life Navigator — cultivation of the integrative and adaptive cortical capacities that allow a person to navigate their life: appraisal, flexible planning, conscious choice, and the accumulated learning of a lifetime, operating through the prefrontal cortex and associated networks. Access is built by brainstorming and embodying qualities such as patience, kindness, discernment, confidence, intuition, resilience, determination, creativity, courage, and resourcefulness, alongside the client’s talents, skills, interests, relationships, accomplishments, and lived examples of completed life tasks—reinforced with MSS.
The Wise Self — cultivation of compassionate, empathic, steady qualities understood as emergent properties of well-regulated cortical networks (medial PFC, ACC, insula) rather than as a separate discrete self. These capacities naturally arise when threat-based activation is not dominating processing. Access is built through felt memories of tenderness, compassion, kindness, clarity, courage, gratitude, and beauty.
Positive Experience Resourcing — activation of real lived moments of joy, connection, accomplishment, awe, and belonging. These memories already have neural representations; the goal is to activate them with enough cortical breadth and depth that they become stronger, more accessible, and more capable of competing with amygdala-linked trauma circuitry. Clinicians are encouraged to listen for positive moments that surface in passing during therapeutic conversation—a proud moment, a laugh, a meaningful connection—and to pause and resource those moments using the NCI prompts.
What the VitalMe app offers for resourcing: personalized Resource Team meditations that incorporate each client’s specific figures, with optional music and nature sounds; a personalized Life Navigator meditation built from the qualities, skills, relationships, and accomplishments the client has identified; Wise Self meditations designed to deepen access to compassionate steady states; and personalized visual resource creation—clients can describe their peaceful place or a resource figure and the app will generate an image that brings that resource to life. Clients can also upload photographs of themselves (at any age) and of real-life resource figures, and the app will create composite images placing them together with their resource or within their peaceful place. These personalized visuals activate the same visual cortical networks each time they are revisited, strengthening the positive circuitry connected to safety, nurturing, and protection.
4.7Imaginal Repair and Memory Reconsolidation
Imaginal repair is the core therapeutic move that NCI inherits from Alison Teal’s Super-Resourcing: once a wounded part is identified, the clinician guides the client in offering that part the missing experiences it needed but never received. The part is met on its own terms—asked what it needs, what was missing, who could have been there, what a different experience would have looked like—and the clinician guides the client to provide that imaginal experience in full, staying with the part until there is a felt sense of safety, regulation, and completeness. This reparative move, pioneered in Super-Resourcing and Parnell’s AF-EMDR, is what NCI takes as the fundamental unit of healing work.
NCI extends this work with structured multi-sensory cortical prompting throughout the repair. The core clinical act is the same—identify the part, offer what was missing—and NCI’s contribution is to widen the cortical surface across which that reparative experience is encoded. The more distributed the activation, the more effectively the new positive circuit can compete with and dilute the narrowly encoded trauma pattern.
When a wounded part has been identified—whether through EMDR’s trace-back technique (informed by Shapiro) or through direct approach from present-day distress (informed by Fisher and Teal)—NCI guides the clinician in offering that part the missing experiences and developmental repair it never received.
NCI supports two pathways for identifying the wounded part. The first is the Trace-Back Technique drawn from EMDR: the clinician begins by identifying the current issue, situation, or trigger that has brought the client’s distress forward. Trigger, emotions, body sensations, and negative cognition are named together. The client is then asked to hold all of these at once and to trace back in time without censoring, allowing whatever arises to come forward. The client typically lands on an earlier experience or a younger part that is being activated by the current trigger—this past experience is the source of what is showing up in the present. Clinicians trained in EMDR may then move into standard EMDR processing with the identified memory or part; clinicians trained in other modalities may use their own approach. In all cases, the NCI resourcing and imaginal repair work proceeds from here, as it builds the positive neural circuitry that creates lasting change regardless of modality.
The second pathway is to identify the wounded part directly through the client’s present-day emotional and physical distress. After grounding to access Awareness, the client is invited to connect with the younger part holding the distress—a sad part, a scared part, a part that feels unworthy, or a part carrying other emotional pain. The clinician asks the client to get a sense of this young part—how old they are, what they are experiencing, the circumstances they are in. Once the wounded part is identified and understood, the clinician proceeds with imaginal repair: offering that part the missing experiences it needs.
In either pathway, the clinician guides the client to check in with the wounded part: “What does this scared part (sad part, angry part) need right now?” “Who could be there to support that need?” “What experience has this part been missing?” “If this part could have had a different experience, what would that look like?” Each missing experience offered—safety, comfort, protection, connection, being seen—activates memory reconsolidation and builds new positive neural circuits connected to the nucleus accumbens. The clinician continues to check in with the part until there is a felt sense of safety, regulation, and completeness.
The neuroscience is direct. Research following Nader, Schafe, and LeDoux’s 2000 discovery demonstrated that reactivated memories require new protein synthesis for restabilization, entering a temporarily labile state during which they can be modified. A critical requirement for triggering this reconsolidation window is prediction error—a mismatch between what the memory predicts and what is currently experienced. NCI’s positive reimagining protocol naturally generates this prediction error: when trauma memories are reactivated but the expected threatening elements are replaced with protective figures and positive outcomes, the mismatch between predicted threat and experienced safety triggers memory destabilization. The reconsolidation window (roughly 10 minutes to 6 hours post-reactivation) opens for therapeutic modification, during which new positive associations can be encoded alongside, and connected to, the original memory trace.
The NCI Noticing Prompts and MSS are applied throughout imaginal repair to create competing positive circuitry that is broader, richer, and more distributed across the cortex than the original trauma encoding. Certain experiences are especially powerful for cortical activation:
Awe engages the salience network, default mode network, and prefrontal cortex simultaneously—it interrupts habitual self-referential processing and opens the brain to new meaning-making, generating a broad cortical response that is uniquely effective at weakening rigid, trauma-based neural patterns.
Connection activates social-relational circuitry—medial PFC, TPJ, mirror neuron system—and releases oxytocin, which directly facilitates neuroplasticity. Because trauma so often occurs in the context of relational rupture, experiences of felt connection are especially potent for rewiring attachment-based wounds.
Surprise triggers a dopaminergic prediction-error response that signals the brain to pay attention and update its model of the world. When something unexpectedly positive happens in the reimagined scene, encoding strength is enhanced—the brain literally learns faster when expectations are violated in a positive direction.
The principle of reciprocal inhibition—detailed in Section 1—underpins the healing mechanism: the amygdala and nucleus accumbens exhibit mutually inhibitory relationships. When positive valence pathways activate the ventral striatum and nucleus accumbens, this activation suppresses amygdala-mediated fear responses. With repeated imaginal repair, the new positive pathway can progressively inhibit the full cascade of amygdala activation that previously produced trauma capture.
4.8Neural Circuit Visualization: Seeing the Brain Change
The brain is capable of remarkable change, but clients rarely get to see that process in action. The VitalMe app’s Neural Circuit Visualization creates a personalized brain video that allows clients to observe, in representational form, how their brain builds new positive circuits connected to the nucleus accumbens as old amygdala-linked trauma pathways weaken.
The video is introduced in session after resourcing and imaginal repair are complete. It visually illustrates how the positive experiences, resources, and corrective emotional moments activated during the session are forming new neural connections—pathways linked to the nucleus accumbens, the brain’s reward and positive-state circuitry. The visualization is accompanied by auditory input drawn from the client’s own responses to the NCI prompts—the words, feelings, and sensations they identified during the session are reflected back, reinforcing the new circuitry through simultaneous visual and auditory activation.
The neuroscience of this intervention is grounded in observational learning and mirror neuron activation. When clients observe neural change happening—even in representational form—the brain engages many of the same networks involved in actually experiencing that change. Paired with the client’s own words as auditory reinforcement, the visualization creates a multi-sensory consolidation experience that deepens the encoding of new positive pathways.
What the VitalMe app adds between sessions: clients revisit their personalized brain video as part of home practice. Each viewing reactivates the positive neural circuitry built during the session—strengthening it through the Hebbian principle of repeated activation. The combination of seeing the brain change and hearing one’s own positive responses provides a uniquely powerful form of neuroplastic reinforcement that supports lasting transformation.
4.9Tour of the Adult Life
Drawing from Janina Fisher’s TIST model, NCI includes a Tour of the Adult Life in which the wounded part is guided through the client’s present-day reality—experiencing the safety, supportive relationships, empowerment, choices, and healthy coping skills that are true now. This activates visual, spatial, relational, emotional, and somatic networks simultaneously. It serves a dual purpose: strengthening the wounded part’s confidence in the safety and stability of the client’s current life, and deepening the part’s trust in the Life Navigator’s ability to care for it.
Neuroscience of the Tour of the Adult Life. Hippocampal time cells and sequential coding neurons organize memories into temporal context, linking experiences that occurred at similar life stages or developmental moments. Traumatic memories are encoded with strong temporal markers that can effectively lock a wounded part at the developmental age of the trauma—so that when a trigger activates any aspect of the memory network, the entire temporal frame reactivates and the part re-experiences the threat as if it were happening now. The brain has no deletion mechanism for these temporal encodings; the pathway out is to build competing temporal associations.
By deliberately guiding the wounded part through present-day visual, spatial, relational, emotional, and somatic input—the current home environment, safe relationships, adult capacities, protective figures, and experiences of choice and agency—the Tour recruits new hippocampal-cortical activity that tags the part with “now” rather than “then.” Each sensory and relational modality activated during the Tour engages a distinct cortical network (visual, auditory, somatosensory, interoceptive, medial PFC for self-reference, temporo-parietal junction for relational processing), creating a broadly distributed present-moment representation that is then temporally linked to the wounded part. With repetition and MSS reinforcement, the temporal retrieval architecture begins to route activation toward the present-day state rather than the traumatic past, progressively disrupting the loop that kept the trauma encoded in present-tense experience.
What the VitalMe app offers: guided exercises that help clients revisit the Tour of the Adult Life between sessions, reinforcing the wounded part’s experience of safety and the Life Navigator’s steady presence, with MSS elements and personalized content drawn from the client’s actual present-day life.
4.10Body Scan
Drawing from EMDR’s body scan phase and from somatic modalities (Sensorimotor Psychotherapy, Somatic Experiencing), NCI incorporates a body scan as a distinct step in the framework. Trauma is stored not only in the brain’s neural circuits but in the body itself—held as tension, constriction, numbness, or activation in the somatosensory cortex and autonomic nervous system. After imaginal repair work is complete, NCI incorporates a gentle body scan to surface any residual distress that may still be encoded in the somatic network.
The client is invited to scan slowly, moving from the top of the head down through the face, neck, shoulders, chest, abdomen, and limbs, noticing any areas of remaining tension, discomfort, or activation.
If distress or tension is present, the clinician approaches the sensation with curiosity rather than trying to eliminate it—this area of the body is carrying something that still needs attention. The client is offered the opportunity to understand and care for what arises:
“What does this area of the body want you to know?”
“What does this sensation need to feel comforted or to heal?”
“If this part of the body could do or experience something right now, what would it want?”
Whatever the client identifies—movement, warmth, release, being held—is provided imaginally, extending the repair process into the somatic network, updating the body’s stored trauma response with new adaptive information and building positive circuitry connected to the nucleus accumbens. As an option for residual activation, the clinician may invite the client to imagine the sensation breaking down into tiny particles, dissolving, drifting downward, and being absorbed into the earth to be composted and transformed—one of many somatic release techniques clinicians can draw on from their own training.
If no distress is present, the body scan becomes a powerful moment to reinforce the positive shifts that have occurred. The client is invited to notice the comfort, calm, and ease in the body—the felt experience of new neural circuitry taking hold—and MSS is used to deepen these sensations. The absence of distress is itself significant: it signals that the autonomic nervous system has shifted from sympathetic activation or dorsal vagal shutdown toward ventral vagal regulation. Helping the client notice and take in this calm reinforces the new somatic baseline, strengthening the body’s own evidence that safety is real and present.
What the VitalMe app offers: a guided body scan exercise with calming music and nature sounds that clients can use between sessions to practice somatic awareness and reinforce the ventral vagal shifts achieved in session.
4.11Associated Memory Strategies: Touchstone Identification and Sequential Integration
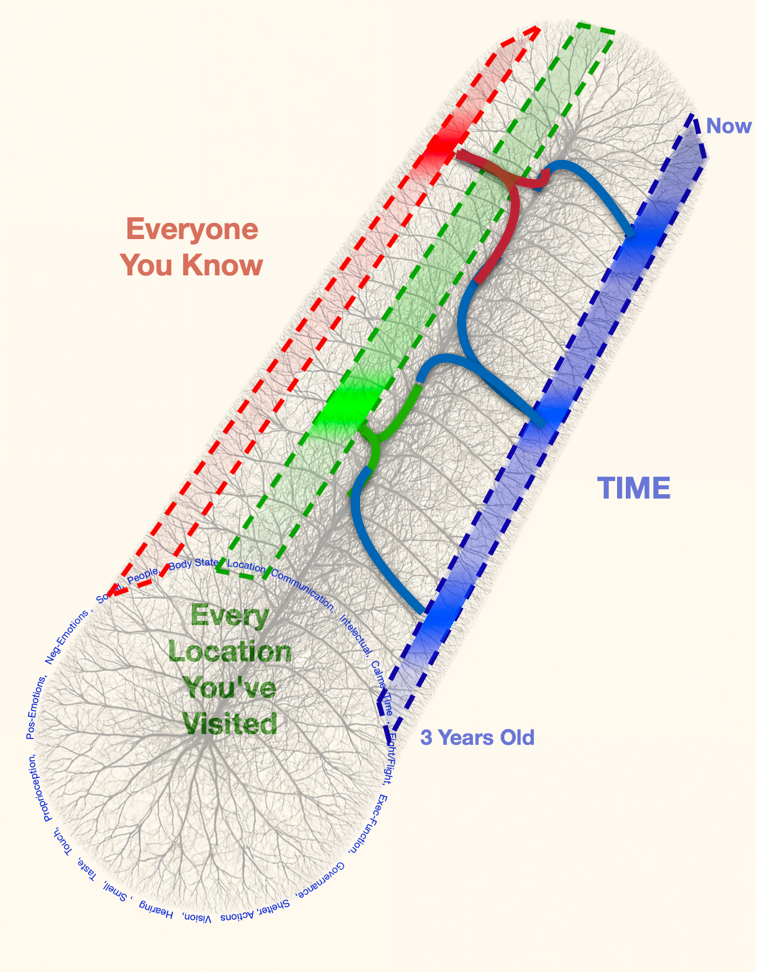
Touchstone Identification. Before processing forward through a full memory network, NCI often begins with Touchstone Identification: the deliberate search for positive counter-experiences whose timeline can overwrite the encoded memory sequence that has trapped the client in a negative mental habit. If a client carries a deeply encoded pattern around the belief “I do not matter,” the clinician helps identify positive experiences throughout their life that represent the opposite—moments of being seen, valued, supported, or loved. Often there is a teacher, neighbor, coach, friend, or meaningful experience that demonstrated care and importance. Clinicians frequently find that clients are surprised by how many counter-experiences exist when they are prompted to look. These memories have not disappeared—they are simply less accessible, because trauma-encoded circuits with strong amygdala connections tend to dominate retrieval and bias perception toward threat-consistent experience. When guided to search deliberately, clients discover a richer landscape of positive experience than they believed existed. This is often a deeply uplifting moment in the therapeutic process. Each positive counter-experience is then activated with the NCI Noticing Prompts and reinforced with MSS, building adaptive neural associations that directly compete with the trauma-encoded circuitry and offering the brain a new pathway out of the habitual negative loop.
Memories are not stored as isolated files. They are organized in associative networks linked by shared emotions, sensations, beliefs, and relational dynamics across different ages and developmental stages (Section 1.9, 1.10). When the brain encodes a wound at age five, that encoding connects to every subsequent experience that activated the same neural pattern—the same fear, the same belief of unworthiness, the same somatic constriction. These linked memories form an associated memory network held together by shared activation in the amygdala and related limbic structures.
Sequential Integration extends imaginal repair across this full network. After the initial wounded part is resourced, the clinician scans forward through the timeline—pausing at each age where the same pattern was reinforced and offering imaginal repair at that node. Hippocampal time cells and sequential coding neurons create temporal context that links related memories; NCI works with this same temporal architecture to build competing neural associations, systematically updating every node in the network.
By the end of this process, the client has not only healed the original wound but has systematically updated every linked memory in the network. The associative links that once reinforced distress now carry a competing narrative of safety, repair, and resilience—building a coherent, integrated sense of self across the full lifespan.
What the VitalMe app offers: guided timeline review exercises with MSS (visual and auditory elements) to revisit and strengthen the positive neural pathways built during timeline work; progress tracking that shows which parts have been resourced, which memory networks have been updated, and where the work is heading; and personalized meditations drawn from the specific positive experiences the client has identified across their lifespan.
4.12Pre-Session Preparation to Maximize Neuroplasticity
Because trauma healing is fundamentally a learning process dependent on neural plasticity, the biological state of the brain at the moment of therapy matters. Section 1’s neuroscience is explicit: learning requires metabolic fuel, particularly glucose and oxygen; memory storage depends on the brain’s capacity to grow new neurons and form new synapses; and anxiety interferes with creativity and learning by consuming metabolic resources. NCI recommends—and the VitalMe app supports—pre-session preparation that optimizes the brain’s capacity for new circuit formation:
Sleep — quality sleep before the session is essential for optimal brain function and neural plasticity; sleep is when the brain consolidates learning through memory re-coding and synaptic strengthening.
Nutrition — a balanced meal of micronutrients within two hours of the session supplies the glucose, oxygen, and metabolites needed to create new neurons and synaptic connections. Without proper fuel, learning and neural integration are inhibited.
Aerobic exercise — 45 minutes of aerobic activity no more than an hour before session substantially increases hippocampal neurogenesis for at least four hours afterward. Moving through visually complex natural environments (forests, parks, trails) activates the visual system and reduces rumination, further preparing the brain.
Dark chocolate — 50 grams of 70%+ cacao no more than 45 minutes prior supports positive neurochemical balance, boosts cognition, and provides glucose for neural growth and plasticity.
Environment — open exterior windows for high oxygen and low CO₂; CO₂ concentrations above 800 ppm can reduce learning by as much as 70%. Fresh air, natural light, and comfortable temperature all support the neuroplastic processes that therapy depends on.
What the VitalMe app offers: personalized sleep meditations to support restful sleep; reminders for nutrition, exercise, and dark chocolate timing aligned with the client’s session schedule; pre-session grounding exercises; and optional mindful-movement prompts for outdoor aerobic preparation.
4.13The VitalMe App: Between-Session Reinforcement
NCI is supported by the VitalMe app, which extends the therapeutic process between sessions by giving clients structured ways to fire and strengthen the new neural pathways built in session. This is the Hebbian principle at work: neurons that fire together wire together, and the more frequently positive pathways are activated, the stronger and more dominant they become. Each revisit of a resourced state, reimagined repair, or practice of mindful awareness is another firing of the new neural pathway—and each firing strengthens it.
The VitalMe app provides:
Preparation support — reminders and guidance for sleep, nutrition, exercise, dark chocolate, and environmental setup
Grounding and regulation exercises — paced breathing (4-4-8, box breathing), vagal toning, humming, hand-on-heart, grounding-cord visualization, extended-exhale breathing
Mindful Awareness practices — guided exercises to develop and deepen the observing presence, with practices that cultivate differentiation between experience and the awareness that notices experience
Personalized Life Navigator meditation — built from the specific qualities, skills, relationships, talents, and accomplishments the client has identified, with optional music and nature sounds
Wise Self meditation — guided practices drawing on the client’s own lived moments of compassion, kindness, courage, and presence to deepen access to these steady cortical states
Personalized Resource Team meditation — incorporating each client’s specific resource figures (protector, nurturer, wise figure, healer, champion, playful figure, peaceful place, compassionate figures) with layered MSS
Visual resource creation — the app generates personalized images of clients’ peaceful places, protective figures, nurturers, and healers from client-provided descriptions. Clients can upload photographs of themselves (at any age) and of real-life resource figures, and the app creates composite images placing them together with their resource or within their peaceful place. These personalized visuals activate the same visual cortical networks each time they are revisited
Neural Circuit Visualization — the personalized brain video reflecting the client’s session content, with accompanying auditory reinforcement drawn from the client’s own NCI prompt responses
MSS and BLS options — bilateral auditory tones, complex binaural soundscapes, visual stimulation (kaleidoscope, forest walks, coastal scenes, path-walking), music and nature sounds, selectable for any resourcing or imaginal work
Timeline review exercises — revisiting positive experiences across the lifespan with MSS support, building the competing positive narrative across the full developmental arc
Tour of the Adult Life — guided exercises to revisit the wounded part’s experience of present-day safety and the Life Navigator’s steady presence
Body scan practice — guided somatic exercises with calming music and nature sounds to reinforce ventral vagal regulation and the client’s own somatic evidence that safety is real and present
Manifestation Guide — structured support for mind-movie creation with music and audio, collaging, and future visualization
Progress tracking — a visual map of the healing journey: parts addressed, remaining wounded parts, positive beliefs integrated, memory networks updated, and where the work is heading
Session Debrief and Follow-Up. A brief debrief at the end of each session helps anchor insights and somatic shifts. Post-session effects—dreams, emotional waves, new memories surfacing—are normalized as signs that neural networks are actively reorganizing. The essential work after session is reinforcement through the VitalMe app, where each revisit of a resourced state, reimagined repair, or practice of mindful awareness is another firing of the new neural pathway, and each firing strengthens it.
The VitalMe app makes reinforcement practice accessible and consistent, extending healing into daily life and accelerating the consolidation of lasting positive circuitry connected to the nucleus accumbens.
4.14Future Creation and Manifestation
With trauma-based circuitry weakened and new positive neural pathways established, NCI includes a future-oriented phase that directs the same neural architecture toward what the client wants to create in their life. Drawing from EMDR’s future templating (informed by Shapiro), manifestation work (informed by Dispenza), and the broader neuroscience of imagination, this phase uses multi-dimensional NCI prompting across visual, auditory, somatic, emotional, cognitive, and relational domains to build prospective neural templates.
The neuroscience of imagining is central. The brain does not fully distinguish between a vividly imagined experience and a lived one—both activate overlapping neural systems, including the hippocampal-cortical networks that construct episodic representations and the prefrontal regions responsible for planning and goal-directed behavior. When a client imagines a desired future as if it is happening now—seeing it, feeling it in the body, hearing the sounds, noticing the emotions—the brain begins building the same neural circuitry it would build if the experience were actually occurring. This is prospective memory in action: the more vivid, multisensory, and emotionally engaged the imagined future, the stronger the prospective neural template becomes, and the more likely the brain is to orient behavior toward making it real. Imagination, in this framework, is not wishful thinking—it is the brain’s mechanism for rehearsing and encoding future possibilities, activating the cortex broadly and strengthening connections to the nucleus accumbens that link positive emotion to forward movement.
The Manifestation phase moves through four stages: identifying hopes and dreams; multi-dimensional future visualization using the full NCI prompting framework; integrating internal resources (the Life Navigator, protector figures, Wise Self) into future scenarios; and multi-modal installation with MSS while the client holds the future vision together with positive body sensations, emotions, and cognitions.
When a client cannot imagine a positive future—or encounters resistance, disbelief, or a sense that they don’t deserve good things—this is clinically important information: a part is blocking the imagining. Rather than pushing through, NCI invites curiosity about the blocking part, returns to imaginal repair to offer what that part needs, and then allows the future vision to open naturally.
What the VitalMe app offers for manifestation: the Manifestation Guide supports continued visualization, mind-movie creation with music and audio, collaging with personalized imagery, and structured revisiting of the future vision. Each engagement with this material activates the prospective neural template and strengthens the connections between present-day resources and future aspirations.
Conclusion
Neural Circuit Integration offers a neuroscience-informed framework for enhancing the trauma-informed modalities clinicians already use. Grounded in the contemporary science of distributed memory encoding, neural plasticity, memory reconsolidation, and the oppositional circuitry between the amygdala and the nucleus accumbens, NCI provides structured strategies for building new positive neural circuits that progressively compete with and weaken the trauma circuits encoded during adversity.
By building on attachment theory, mindfulness, polyvagal and somatic approaches, EMDR and its attachment-focused adaptations, and ego state and parts work—and by adding multi-sensory stimulation, the NCI Noticing Prompts, imaginal repair with memory reconsolidation, Neural Circuit Visualization, Tour of the Adult Life, Sequential Integration, pre-session preparation, and the VitalMe app for between-session reinforcement—NCI supports clinicians in deepening their practice and supporting clients in lasting transformation.
NCI affirms the principle that trauma healing does not need to be retraumatizing. With imagination, mindfulness, and integrative wisdom, the nervous system can rewire itself toward health, hope, and meaning. For trauma survivors, NCI offers a path to healing that is gentle, empowering, and transformative.